We offer a range of clinics and services here at Crown Street Surgery to help manage chronic diseases.
Chronic Heart Disease
The most common symptoms of coronary heart disease (CHD) are chest pains (angina) and a heart attack.
You can also experience other symptoms, such as palpitations and unusual breathlessness. In some cases, people may not show any symptoms before they are diagnosed.
Angina
If your coronary arteries become partially blocked, it can cause chest pain (angina). This can be a mild, uncomfortable feeling similar to indigestion.
However, a severe angina attack can cause a painful feeling of heaviness or tightness, usually within the centre of the chest, which may then spread to the arms, neck, jaw, back or stomach.
Angina attacks are often triggered by physical activity or stressful situations. Although symptoms of Angina usually pass within 10 minutes, you can alleviate the symptoms by resting or using a nitrate tablet or spray.
Heart attacks
If your arteries become completely blocked, it can cause a heart attack (myocardial infarction). Heart attacks can cause permanent damage to the heart muscle and, if not treated straight away, can be fatal.
Although symptoms can vary, the discomfort or pain of a heart attack is usually similar to that of angina but often more severe. During a heart attack you may also experience the following symptoms:
Sweating
Light-headedness
Nausea
Breathlessness
The symptoms of a heart attack can be similar to indigestion. For example, they may include a feeling of heaviness in your chest, a stomach ache or heartburn. However, these symptoms can also be accompanied by a pain that affects the arms (particularly the left arm), the neck and the jaw.
A heart attack can happen at any time, including while you are resting. If heart pains last longer than 15 minutes, it may be the start of a heart attack.
Unlike angina, the symptoms of a heart attack are not usually relieved using a nitrate tablet or spray.
In some cases, you may have a heart attack without any symptoms, called a silent myocardial infarction. This is more common in people with diabetes.
Heart failure
Heart failure can also occur in people with CHD when the heart becomes too weak to pump blood around the body, which can cause fluid to build up in the lungs that makes it increasingly difficult to breathe.
Heart failure can happen suddenly (acute heart failure) or gradually over time (chronic heart failure).
Useful links:
British Heart Foundation – Angina
British Heart Foundation – Cardiovascular Disease
British Heart Foundation – Heart Attack
You can also experience other symptoms, such as palpitations and unusual breathlessness. In some cases, people may not show any symptoms before they are diagnosed.
Angina
If your coronary arteries become partially blocked, it can cause chest pain (angina). This can be a mild, uncomfortable feeling similar to indigestion.
However, a severe angina attack can cause a painful feeling of heaviness or tightness, usually within the centre of the chest, which may then spread to the arms, neck, jaw, back or stomach.
Angina attacks are often triggered by physical activity or stressful situations. Although symptoms of Angina usually pass within 10 minutes, you can alleviate the symptoms by resting or using a nitrate tablet or spray.
Heart attacks
If your arteries become completely blocked, it can cause a heart attack (myocardial infarction). Heart attacks can cause permanent damage to the heart muscle and, if not treated straight away, can be fatal.
Although symptoms can vary, the discomfort or pain of a heart attack is usually similar to that of angina but often more severe. During a heart attack you may also experience the following symptoms:
Sweating
Light-headedness
Nausea
Breathlessness
The symptoms of a heart attack can be similar to indigestion. For example, they may include a feeling of heaviness in your chest, a stomach ache or heartburn. However, these symptoms can also be accompanied by a pain that affects the arms (particularly the left arm), the neck and the jaw.
A heart attack can happen at any time, including while you are resting. If heart pains last longer than 15 minutes, it may be the start of a heart attack.
Unlike angina, the symptoms of a heart attack are not usually relieved using a nitrate tablet or spray.
In some cases, you may have a heart attack without any symptoms, called a silent myocardial infarction. This is more common in people with diabetes.
Heart failure
Heart failure can also occur in people with CHD when the heart becomes too weak to pump blood around the body, which can cause fluid to build up in the lungs that makes it increasingly difficult to breathe.
Heart failure can happen suddenly (acute heart failure) or gradually over time (chronic heart failure).
Useful links:
British Heart Foundation – Angina
British Heart Foundation – Cardiovascular Disease
British Heart Foundation – Heart Attack
Diabetes
Click here to see our T2DM leaflet.
Click here to see information on SGLT2 medication potential side effects
Diabetes is a long-term condition caused by too much glucose, a type of sugar, in the blood. It is also known as diabetes mellitus.There are two main types of diabetes, which are explained below:
Type I diabetes
Type II diabetes
Normally, the amount of sugar in the blood is controlled by a hormone called insulin, which is produced by the pancreas. The pancreas is a gland behind the stomach. When food is digested and enters your bloodstream, insulin moves any glucose out of the blood and into cells, where it is broken down to produce energy.
However, in people with diabetes, the body is unable to break down glucose into energy. This is because there is either not enough insulin to move the glucose, or because the insulin that is there does not work properly.
Our specialist diabetes team will provide you with support, regular reviews and the day-to-day care of your needs.
All Diabetic patients are entitled to an annual review. The Practice will normally contact you if yours is due. The review takes place in two parts – a data collection appointment and where appropriate, a follow up care plan appointment. If you feel you have been missed, or require a more urgent review, then please contact the Practice to arrange an appointment.
At the initial data collection appointment, your blood pressure, weight, urine, feet and well-being will be checked. It is necessary for you to bring an early morning urine sample with you. Following your initial appointment you’ll be offered a ‘Face to Face’ appointment or a Telephone Consultation with a diabetic specialist nurse to discuss your results and issue you with a care plan booklet.
For more information please visit the websites below:
Useful links
Diabetes UK
Hypertension
Hypertension relates to High Blood Pressure.
High blood pressure often causes no symptoms, or immediate problems, but it is a major risk factor for developing a serious cardiovascular disease (conditions that affect the functioning of the heart and the circulation of blood around the body), such as a stroke or heart disease.
Useful links
NHS Choices – High Blood Pressure Explained
Blood Pressure Association
British Heart Foundation
British Hypertension Society
High blood pressure often causes no symptoms, or immediate problems, but it is a major risk factor for developing a serious cardiovascular disease (conditions that affect the functioning of the heart and the circulation of blood around the body), such as a stroke or heart disease.
Useful links
NHS Choices – High Blood Pressure Explained
Blood Pressure Association
British Heart Foundation
British Hypertension Society
Respiratory
Our respiratory clinics are primarily intended for patients with Asthma and COPD.
Asthma is caused by inflammation of the airways. These are the small tubes, called bronchi, which carry air in and out of the lungs. If you have asthma, the bronchi will be inflamed and more sensitive than normal. Our practice nurses have specialist asthma qualifications. During their clinics they monitor your overall condition, offer advice, answer any queries and ensure your treatment is effective.
Chronic obstructive pulmonary disease (COPD) is the name for a collection of lung diseases including chronic bronchitis, emphysema and chronic obstructive airways disease. People with COPD have trouble breathing in and out. This is referred to as airflow obstruction. Breathing difficulties are caused by long-term damage to the lungs, usually because of smoking.
Asthma and COPD Clinics
We hold clinics to diagnose and to help patients to manage their asthma or COPD.
We like to see all our patients who have been diagnosed with these conditions at least once a year, depending on the severity of your condition, we may invite you to come to the clinic more often in order to ensure we give you the care you require.
Useful links
NHS Choices – Asthma
The British Lung Foundation
Asthma UKNHS Choices – COPD
Asthma is caused by inflammation of the airways. These are the small tubes, called bronchi, which carry air in and out of the lungs. If you have asthma, the bronchi will be inflamed and more sensitive than normal. Our practice nurses have specialist asthma qualifications. During their clinics they monitor your overall condition, offer advice, answer any queries and ensure your treatment is effective.
Chronic obstructive pulmonary disease (COPD) is the name for a collection of lung diseases including chronic bronchitis, emphysema and chronic obstructive airways disease. People with COPD have trouble breathing in and out. This is referred to as airflow obstruction. Breathing difficulties are caused by long-term damage to the lungs, usually because of smoking.
Asthma and COPD Clinics
We hold clinics to diagnose and to help patients to manage their asthma or COPD.
We like to see all our patients who have been diagnosed with these conditions at least once a year, depending on the severity of your condition, we may invite you to come to the clinic more often in order to ensure we give you the care you require.
Useful links
NHS Choices – Asthma
The British Lung Foundation
Asthma UKNHS Choices – COPD
Chronic Kidney Disease
What is Chronic Kidney Diseases (CKD)?
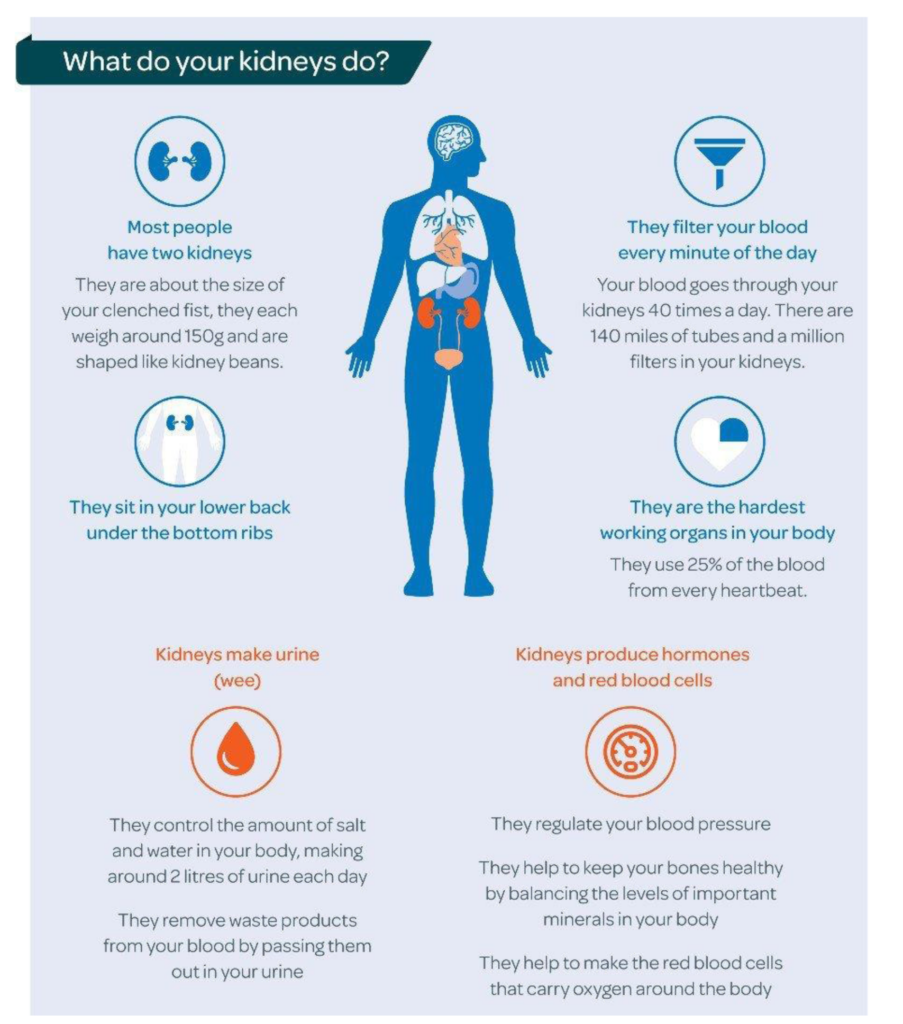
Chronic kidney disease (CKD) is common: around one in 10 people are affected. A diagnosis of chronic kidney disease (CKD) means that your kidneys do not work as well as they should. The term ‘chronic’ means that it is a long-term condition. It does not mean that the condition is severe. Most people with CKD have very mild or no symptoms and are managed long term by their GP.
If you have CKD, your kidneys do not work as well as they should. Damage to your kidneys’ filter system lets blood and protein leak into your urine. Waste products can start to build up in your body as your kidneys can’t remove them properly.
“The good news about being diagnosed early is that we can slow further damage with a combination of highly effective new drug treatments and diet and lifestyle changes. Most people with CKD are able to live full and active lives and feel well.”
How is CKD diagnosed?
CKD is usually diagnosed by blood and urine tests. You may have these tests as part of a routine check-up at your GP surgery or because you are at increased risk of developing CKD because you have other conditions such as diabetes, high blood pressure or heart disease, or a family history of kidney disease.
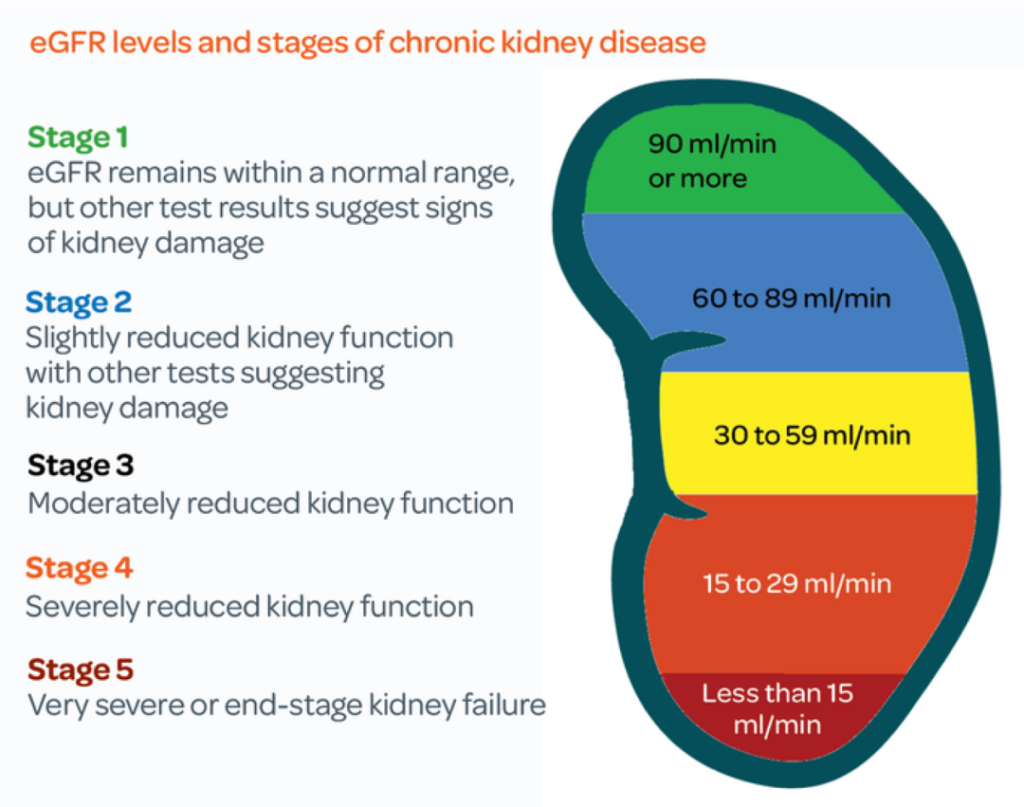
Your doctor, nurse, or health care assistant will carry out a blood test that measures levels of a waste product called creatinine in your blood. They look at the results of this, along with your age, size, ethnic group and gender, to calculate how much waste your kidneys are filtering every minute. The calculation is called your estimated glomerular filtration rate, usually shortened to eGFR. Healthy kidneys should be able to filter more than 90ml/min. To get a fuller picture of your kidney function, doctors will also carry out tests on your urine to look for blood and protein, which can be present if your kidneys aren’t working properly.
CKD is then categorised into FIVE “stages” based on these blood & urine test results. The five stages of CKD range from being at risk (stage 1) through to kidney failure (stage 5). But only around 1 in 100 people with CKD ends up with kidney failure. Most people with CKD Stages 1 – 3 manage the condition themselves with support from their GP. With treatment and lifestyle changes, lots of people stay stable and their CKD doesn’t get worse.
How did I get CKD?
Several factors can affect whether you’ll develop CKD. These include:
Ageing: The rate at which blood passes through the blood vessels in the kidney each minute drops as you get older as a normal part of ageing. CKD can happen at any age, but kidney function begins to fall by approximately 1 per cent per year after the age of 40. However, your kidney function may never fall as low as the threshold to be classed as CKD.
High blood pressure: High blood pressure (hypertension) can constrict and narrow blood vessels in the kidneys, causing damage
Diabetes: Diabetes that isn’t well-controlled can damage blood vessels in the kidneys. This can lead to high blood pressure, which can further damage the kidneys.
Genetics: Some people are more prone to CKD due to their genes. Some may have inherited kidney diseases, such as polycystic kidneys, but for other people it is a combination of different factors that put them at risk
Autoimmune diseases: Some autoimmune conditions, such as lupus can increase the likelihood of developing CKD. We don’t fully understand why
Lifestyle factors: Some lifestyle factors, such as being overweight, can put more pressure on the kidneys and they have to work overtime.
How is CKD treated?
We can’t reverse kidney damage that has already happened; however, we can help stop it getting any worse with drug treatments and lifestyle changes.
If you have mild CKD (stages one to three) and your kidney function is stable, you will be monitored by your GP practice.
What will my GP do?
You will have annual checks with your GP, or practice nurse, to monitor your condition and overall health. At each visit you will have your weight and blood pressure measured and a sample of your urine will be checked for signs of blood, protein or infection. You will have a blood test to measure your kidney function and check for signs of anaemia. Your healthcare professional will discuss any symptoms you may be having and whether any treatment is needed. You will be screened for other conditions, like Diabetes, Hypertension (high blood pressure), and high cholesterol, as managing these conditions will improve your kidney health in the long term.
Some people may have more frequent monitoring if they have recently been unwell or admitted to hospital, if they are changing or starting new medication, or if they have had a recent decline in kidney function.
Medication
You may need to take medication to reduce your blood pressure or control your diabetes. These conditions can make your CKD worse if uncontrolled as they damage blood vessels in the kidneys.
For anyone with CKD stage 3-5, a statin is recommended. This should be discussed with your GP, or a pharmacist. This is recommended even if your cholesterol level is ok, or your QRISK score (risk of having a heart attack or stroke in 10 years) is ok. Reducing cholesterol protects the blood vessels in the kidney, and statins also have anti-inflammatory effects which are kidney-protective.
NICE recommends that people with CKD who either have diabetes, or protein in their urine are prescribed SGLT2 inhibitor drugs which can help to slow down CKD progression and have also been shown to reduce your chances of having a heart attack or stroke. In addition, those with diabetes already on an SGLT2 inhibitor can sometimes be offered an additional drug called finerenone (a non-steroidal mineralocorticoid receptor).
If you have Severe CKD (stages four to five) you will be referred to a specialist (nephrologist). Your specialist will give you support and advice to help you understand your treatment options, which may include dialysis, a kidney transplant or conservative care. Some foods that are high in salt, potassium and phosphate can be harmful to your kidneys. Your kidney team will tell you if you need to lower the amount of potassium in your diet. A dietitian can give you specialist advice on how you can adapt your diet if needed.
What can I do to keep healthy?
Eat a healthy balanced diet.
Take regular exercise. This can be as simple as increasing the amount of walking that you do each day. Doing any amount of exercise is better than doing none. Your GP can give you advice about how to exercise safely.
Give up smoking. Your GP can help you with this.
Give up or cut down on your alcohol intake.
Keep up to date with your vaccinations. When you have kidney disease, you are more likely to get other illnesses and take longer to recover. This can make your kidney function worse, so it is important to get treatment early. Ask your GP about having flu, pneumonia and Covid-19 vaccinations.
Check your blood pressure regularly. Your GP can teach you how to do this yourself at home.
Some over-the-counter and prescription medicines can make your kidney disease worse. Always tell your doctor and pharmacist that you have kidney disease and check that the medication you are given is safe to take.
Do not stop any medication without taking medical advice.
For more detailed healthy eating and lifestyle advice: https://kidneycareuk.org/get-support/healthy-diet-support/healthy-eating-and-lifestyle-for-your-kidneys/
What if I have more questions?
You can contact us at Crown Street Surgery where one of our expert team of GPs, pharmacists, and advanced nurse practitioners will be able to help you.
You can also find out more information online, but please make sure to only visit trusted sites with good quality information, such as the NHS website and Kidney Care UK
https://www.nhs.uk/conditions/kidney-disease/
https://kidneycareuk.org/
https://www.kidney.org.uk/chronic-kidney-disease
https://www.kidneyresearchuk.org/conditions-symptoms/chronic-kidney-disease/
Click here to see information on SGLT2 medication potential side effects
Click here to see information on Sick Day Medications
Chronic kidney disease (CKD) is common: around one in 10 people are affected. A diagnosis of chronic kidney disease (CKD) means that your kidneys do not work as well as they should. The term ‘chronic’ means that it is a long-term condition. It does not mean that the condition is severe. Most people with CKD have very mild or no symptoms and are managed long term by their GP.
If you have CKD, your kidneys do not work as well as they should. Damage to your kidneys’ filter system lets blood and protein leak into your urine. Waste products can start to build up in your body as your kidneys can’t remove them properly.
“The good news about being diagnosed early is that we can slow further damage with a combination of highly effective new drug treatments and diet and lifestyle changes. Most people with CKD are able to live full and active lives and feel well.”
How is CKD diagnosed?
CKD is usually diagnosed by blood and urine tests. You may have these tests as part of a routine check-up at your GP surgery or because you are at increased risk of developing CKD because you have other conditions such as diabetes, high blood pressure or heart disease, or a family history of kidney disease.
Your doctor, nurse, or health care assistant will carry out a blood test that measures levels of a waste product called creatinine in your blood. They look at the results of this, along with your age, size, ethnic group and gender, to calculate how much waste your kidneys are filtering every minute. The calculation is called your estimated glomerular filtration rate, usually shortened to eGFR. Healthy kidneys should be able to filter more than 90ml/min. To get a fuller picture of your kidney function, doctors will also carry out tests on your urine to look for blood and protein, which can be present if your kidneys aren’t working properly.
CKD is then categorised into FIVE “stages” based on these blood & urine test results. The five stages of CKD range from being at risk (stage 1) through to kidney failure (stage 5). But only around 1 in 100 people with CKD ends up with kidney failure. Most people with CKD Stages 1 – 3 manage the condition themselves with support from their GP. With treatment and lifestyle changes, lots of people stay stable and their CKD doesn’t get worse.
How did I get CKD?
Several factors can affect whether you’ll develop CKD. These include:
Ageing: The rate at which blood passes through the blood vessels in the kidney each minute drops as you get older as a normal part of ageing. CKD can happen at any age, but kidney function begins to fall by approximately 1 per cent per year after the age of 40. However, your kidney function may never fall as low as the threshold to be classed as CKD.
High blood pressure: High blood pressure (hypertension) can constrict and narrow blood vessels in the kidneys, causing damage
Diabetes: Diabetes that isn’t well-controlled can damage blood vessels in the kidneys. This can lead to high blood pressure, which can further damage the kidneys.
Genetics: Some people are more prone to CKD due to their genes. Some may have inherited kidney diseases, such as polycystic kidneys, but for other people it is a combination of different factors that put them at risk
Autoimmune diseases: Some autoimmune conditions, such as lupus can increase the likelihood of developing CKD. We don’t fully understand why
Lifestyle factors: Some lifestyle factors, such as being overweight, can put more pressure on the kidneys and they have to work overtime.
How is CKD treated?
We can’t reverse kidney damage that has already happened; however, we can help stop it getting any worse with drug treatments and lifestyle changes.
If you have mild CKD (stages one to three) and your kidney function is stable, you will be monitored by your GP practice.
What will my GP do?
You will have annual checks with your GP, or practice nurse, to monitor your condition and overall health. At each visit you will have your weight and blood pressure measured and a sample of your urine will be checked for signs of blood, protein or infection. You will have a blood test to measure your kidney function and check for signs of anaemia. Your healthcare professional will discuss any symptoms you may be having and whether any treatment is needed. You will be screened for other conditions, like Diabetes, Hypertension (high blood pressure), and high cholesterol, as managing these conditions will improve your kidney health in the long term.
Some people may have more frequent monitoring if they have recently been unwell or admitted to hospital, if they are changing or starting new medication, or if they have had a recent decline in kidney function.
Medication
You may need to take medication to reduce your blood pressure or control your diabetes. These conditions can make your CKD worse if uncontrolled as they damage blood vessels in the kidneys.
For anyone with CKD stage 3-5, a statin is recommended. This should be discussed with your GP, or a pharmacist. This is recommended even if your cholesterol level is ok, or your QRISK score (risk of having a heart attack or stroke in 10 years) is ok. Reducing cholesterol protects the blood vessels in the kidney, and statins also have anti-inflammatory effects which are kidney-protective.
NICE recommends that people with CKD who either have diabetes, or protein in their urine are prescribed SGLT2 inhibitor drugs which can help to slow down CKD progression and have also been shown to reduce your chances of having a heart attack or stroke. In addition, those with diabetes already on an SGLT2 inhibitor can sometimes be offered an additional drug called finerenone (a non-steroidal mineralocorticoid receptor).
If you have Severe CKD (stages four to five) you will be referred to a specialist (nephrologist). Your specialist will give you support and advice to help you understand your treatment options, which may include dialysis, a kidney transplant or conservative care. Some foods that are high in salt, potassium and phosphate can be harmful to your kidneys. Your kidney team will tell you if you need to lower the amount of potassium in your diet. A dietitian can give you specialist advice on how you can adapt your diet if needed.
What can I do to keep healthy?
Eat a healthy balanced diet.
Take regular exercise. This can be as simple as increasing the amount of walking that you do each day. Doing any amount of exercise is better than doing none. Your GP can give you advice about how to exercise safely.
Give up smoking. Your GP can help you with this.
Give up or cut down on your alcohol intake.
Keep up to date with your vaccinations. When you have kidney disease, you are more likely to get other illnesses and take longer to recover. This can make your kidney function worse, so it is important to get treatment early. Ask your GP about having flu, pneumonia and Covid-19 vaccinations.
Check your blood pressure regularly. Your GP can teach you how to do this yourself at home.
Some over-the-counter and prescription medicines can make your kidney disease worse. Always tell your doctor and pharmacist that you have kidney disease and check that the medication you are given is safe to take.
Do not stop any medication without taking medical advice.
For more detailed healthy eating and lifestyle advice: https://kidneycareuk.org/get-support/healthy-diet-support/healthy-eating-and-lifestyle-for-your-kidneys/
What if I have more questions?
You can contact us at Crown Street Surgery where one of our expert team of GPs, pharmacists, and advanced nurse practitioners will be able to help you.
You can also find out more information online, but please make sure to only visit trusted sites with good quality information, such as the NHS website and Kidney Care UK
https://www.nhs.uk/conditions/kidney-disease/
https://kidneycareuk.org/
https://www.kidney.org.uk/chronic-kidney-disease
https://www.kidneyresearchuk.org/conditions-symptoms/chronic-kidney-disease/
Click here to see information on SGLT2 medication potential side effects
Click here to see information on Sick Day Medications